Benzodiazepines share a common mechanism of action, yet patients and clinicians consistently observe that they can feel markedly different in practice.
These differences are not subjective anomalies — they are rooted in pharmacokinetics: how the drug is absorbed, distributed, metabolized, and eliminated. Understanding these distinctions is essential when considering PRN prescribing, daily dosing strategies, crossovers, and tapering.
Below is a clinically grounded but practical explanation of why these medications vary so noticeably.
Pharmacokinetics Vary Substantially Across the Class
Pharmacokinetic characteristics among the benzodiazepines differ considerably.
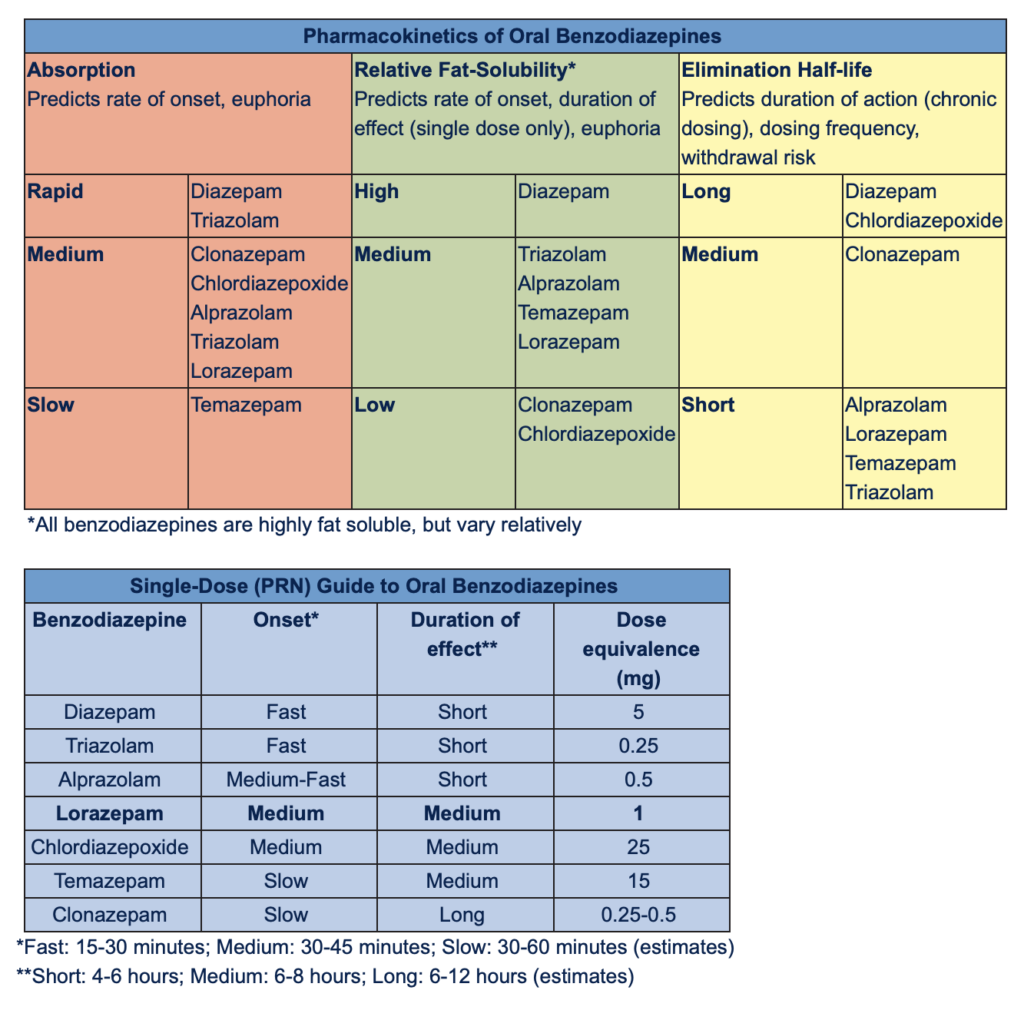
Diazepam has the highest absorption rate and the greatest degree of fat solubility in the class. This combination produces exceptionally rapid onset of action and is associated with a higher risk of euphoria due to swift central nervous system penetration.
In general, medications that enter the brain more rapidly tend to have greater reinforcing potential.
Fat Solubility and Redistribution: Why Effects May Fade Quickly
The most fat-soluble benzodiazepines rapidly redistribute to adipose tissue after their initial central nervous system exposure. While this redistribution does not mean the drug has been eliminated, it does reduce the concentration in the brain.
Clinically, this results in a quicker offset of acute effects.
This explains a common paradox:
The acute effects of a single dose of diazepam are typically of shorter duration than lorazepam — despite diazepam having a substantially longer elimination half-life.
This phenomenon is frequently misunderstood. The subjective duration of effect from a single dose is heavily influenced by redistribution, not just elimination.
Terminal Half-Life Does Not Predict Acute Duration
The half-life reported for benzodiazepines refers to the terminal half-life — the time required for elimination after the drug has equilibrated with adipose tissue.
Importantly, terminal half-life does not predict the acute duration of action.
A medication can have:
- A long terminal half-life
- Yet a relatively brief single-dose calming window
This distinction is central to understanding why two benzodiazepines with very different half-lives may feel similar — or even reversed — in perceived duration after one dose.
What Happens With Chronic Dosing?
The clinical picture shifts significantly when benzodiazepines are dosed regularly.
With chronic administration, long half-life agents such as diazepam accumulate gradually over several weeks. This accumulation leads to more stable plasma concentrations and more durable anxiolysis over 24 hours, often allowing for once-daily dosing.
In contrast, shorter half-life agents do not accumulate to the same extent, which may increase the risk of:
- Interdose withdrawal
- Rebound symptoms
- More frequent dosing requirements
Thus, while diazepam may feel shorter acting after a single dose, it behaves very differently when used daily.
The gradual accumulation and stabilization of plasma concentrations seen with long half-life benzodiazepines can facilitate tapering by reducing peak–trough fluctuations, minimizing interdose withdrawal, and allowing for more tolerable dose reductions over time.
Active Metabolites Extend Elimination
Several benzodiazepines — most notably chlordiazepoxide and diazepam — have active metabolites that contribute to a very long overall elimination half-life.
These metabolites (including nordiazepam) remain pharmacologically active and significantly extend total drug exposure.
Other agents such as alprazolam, clonazepam, and lorazepam do not rely on these same long-acting metabolites in the same way, which further differentiates their pharmacokinetic profiles.
Urine Drug Screening: Why False Negatives Occur
The majority of clinically available benzodiazepines are eventually metabolized to nordiazepam or oxazepam — the primary metabolites detected in standard urine immunoassays.
However, alprazolam, clonazepam, and lorazepam are exceptions. These medications often demonstrate false-negative results on routine urine drug screens unless confirmatory testing with mass spectrometry is performed.
This is a common source of confusion in clinical practice and can lead to incorrect assumptions about adherence.
PRN (As-Needed) Use: Trade-Offs in Speed and Duration
Benzodiazepines are frequently used on an as-needed (PRN) basis for anxiety or insomnia.
For acute anxiolysis, a faster onset of action is typically preferred. However, rapid onset often comes with:
- Potentially increased euphoria
- Shorter duration of effect (approximately 4–6 hours)
Lorazepam is often selected as a PRN option because of its “middle-of-the-road” characteristics — offering relatively reliable onset and duration without the extreme rapidity of diazepam or alprazolam.
The Clinical Takeaway
- Diazepam has a rapid absorption rate and high fat solubility, leading to rapid onset and greater euphoric potential.
- Highly fat-soluble benzodiazepines redistribute quickly into adipose tissue, shortening acute subjective duration.
- Terminal half-life reflects elimination after tissue equilibration and does not predict single-dose effect duration.
- Long half-life agents accumulate with chronic dosing, producing steadier 24-hour anxiolysis.
- Active metabolites (e.g., nordiazepam) extend elimination time for certain agents.
- Standard urine drug screens may not reliably detect alprazolam, clonazepam, or lorazepam without confirmatory testing.
- Faster PRN agents typically provide quicker relief but shorter duration and potentially greater reinforcement risk.
Benzodiazepines may share a receptor target, but their pharmacokinetics shape dramatically different lived experiences. Understanding these nuances is essential for thoughtful prescribing, safe tapering, and accurate clinical interpretation.
This information on benzodiazepine pharmacokinetics and clinical characteristics was adapted from The Psychopharmacology Blue Book: Outpatient Practice Companion by Bryan Shapiro, MD (LWW, published October 13, 2025). The Psychopharmacology Blue Book is a concise clinical drug reference that summarizes pharmacologic properties, effects, and use considerations for psychotropic medications.